 DIET & NUTRITION
DIET & NUTRITION  PATIENT EDUCATION
PATIENT EDUCATION  OBESITY/WEIGHT MANAGEMENT
OBESITY/WEIGHT MANAGEMENT  EXERCISE/TRAINING
EXERCISE/TRAINING  LEGAL MATTERS
LEGAL MATTERS  GUIDELINES/RECOMMENDATIONS
GUIDELINES/RECOMMENDATIONS Based on these data, can you diagnose this perplexing case that eludes common respiratory diseases?
Investigating the cause of severe dyspnea and dry cough in a young male smoker presents an interesting diagnostic challenge. This patient’s symptoms are coupled with key findings including bilateral inspiratory crackles, hypoxemia after physical exertion, reticular shadows in both lungs on a chest X-ray, mild pulmonary hypertension on echocardiography, and a chest CT showing upper-lobes predominant bizarre shaped cysts with scattered lung nodules.
Key Data:
- A 24-year-old male active smoker presents with dyspnea on exertion, and dry cough lasting 4 months. The patient cannot walk more than 100m on flat ground without stopping for breath.
- Physical examination reveals bilateral inspiratory crackles, and significant hypoxemia (SPO2 84%) after climbing 2 flights of stairs.
- Chest X-ray shows reticular shadows in both lungs.
- Echocardiography shows normal left ventricular function, normal valves, with mild pulmonary hypertension.
- Pulmonary function tests show mild restriction with mild reduction in diffusion capacity.
- Routine chemistry is within normal limits.
- Chest CT reveals bilateral upper-lobes predominant bizarre shaped cysts with scattered lung nodules.
- Bronchoscopy and bronchoalveolar lavage (BAL) show no evidence of S-100 and CD-1a.
Question for Evaluation
Based on the data presented, what is the most probable diagnosis?
- Metastatic malignancy
- Pulmonary Langerhans cell histiocytosis (PLCH)
- Lymphocytic interstitial pneumonitis
- Atypical infection
Pulmonology Latest Posts
- EULAR/PReS Recommendations for the Diagnosis and Management of Still’s Disease, Comprising Systemic Juvenile Idiopathic Arthritis and Adult-Onset Still’s Disease
- Advanced Polysomnography Feature Engineering and Machine Learning Improve Differentiation of Central Hypersomnolence Disorders
- A Breath of Uncertainty: Diagnostic Challenge in a Young Athlete
- GINA 2026 Update: Asthma Management in Primary Care, Biologic Updates, and More
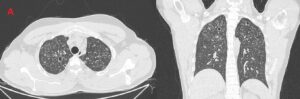
Bilateral upper-lobes predominant bizarre shaped cysts with scattered lung nodules.